Best Hospital in Ghatkopar, Mumbai | Zynova Shalby Hospital


Ovarian Cancer Symptoms in Women | Early Signs Mumbai
- Home
- Ovarian Cancer Symptoms in Women: Early Warning Signs You Should Not Ignore
- admin
- 0 Comments
In 2022 alone, India recorded 47,333 new cases of ovarian cancer and 32,978 deaths from the disease. That is roughly one death every sixteen minutes from a cancer that, when caught early, has a survival rate above 90 percent.
The problem is not a lack of treatment. The problem is timing. Approximately 70 to 80 percent of Indian women with ovarian cancer are diagnosed at an advanced stage, when the cancer has already spread well beyond the ovaries. By that point, treatment becomes far more complex and outcomes far less predictable.
This happens because the early signs of ovarian cancer are quiet. They feel like everyday discomfort. A little bloating. Some lower back pain. Feeling full too quickly. Most women wait months before they mention these symptoms to a doctor, and many doctors dismiss them the first time around.
This blog covers everything women in Mumbai and across India need to know: the warning signs, the risk factors, ovarian cancer stages with real survival data, ovarian cancer diagnosis steps including the CA-125 test, treatment options, prevention, diet, and how to find the right ovarian cancer specialist doctor in Mumbai.
What Is Ovarian Cancer?
Ovarian cancer in women starts in the ovaries, the two almond-shaped glands on either side of the uterus that produce eggs and hormones like estrogen and progesterone. When cells in or near the ovaries begin to grow abnormally and multiply without control, they form a tumor. Left untreated, these cells can spread through the abdomen, pelvis, and to distant organs.
There are three main types:
Epithelial ovarian cancer is the most common, accounting for 85 to 90 percent of all cases. It starts in the cells covering the outer surface of the ovaries.
Germ cell tumors develop from the egg-producing cells and are more common in younger women and girls.
Stromal tumors start in the hormone-producing cells of the ovary and are rare, representing about 7 percent of cases.
The ovaries sit deep inside the pelvis, which means tumors can grow to a significant size before they create symptoms obvious enough to act on. This is one of the core reasons why ovarian cancer is called the silent killer. The body does send signals. But those signals are easy to mistake for digestive problems, period-related discomfort, or general fatigue.
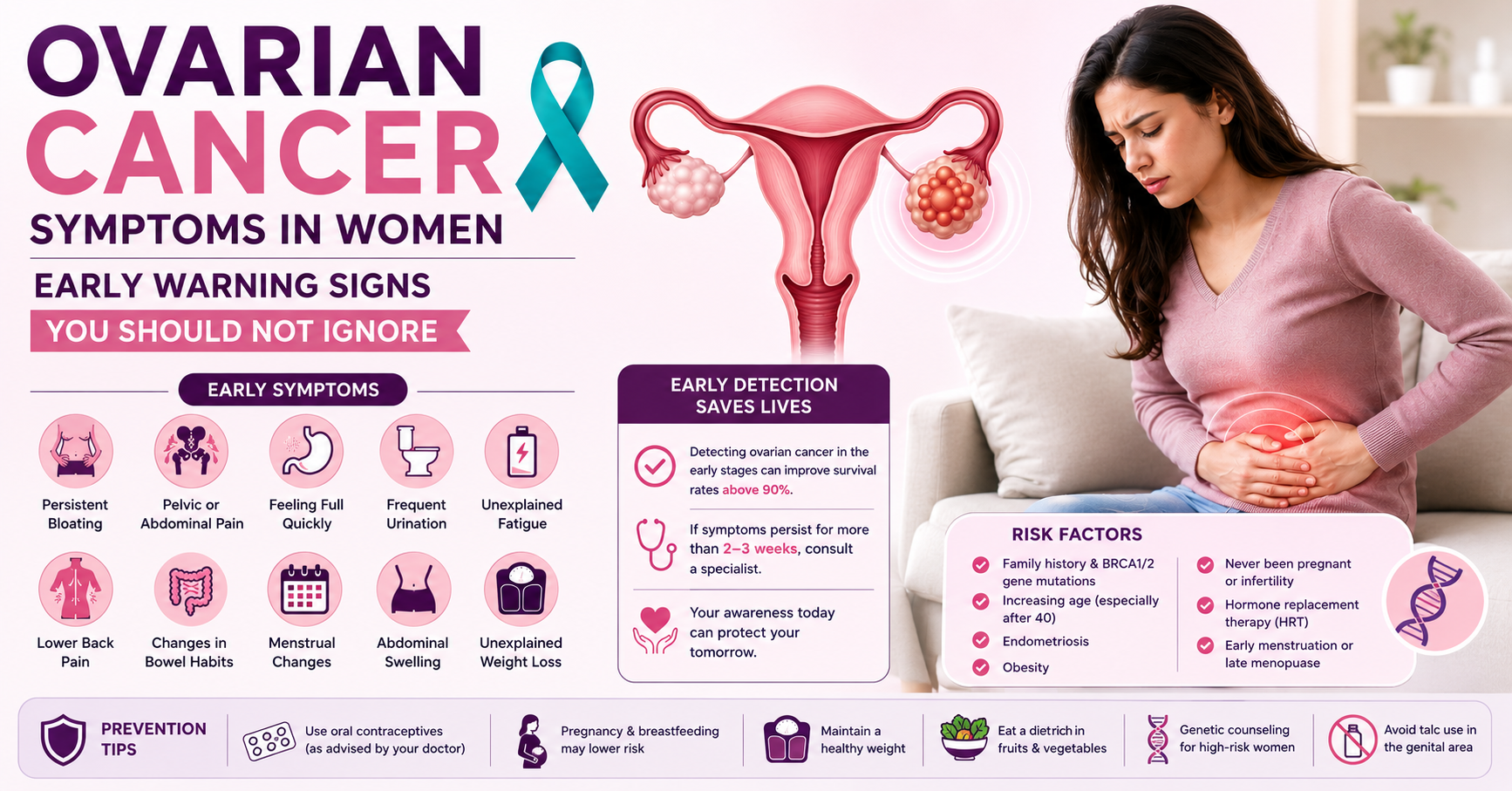
Ovarian Cancer Symptoms: The Complete List of Early Warning Signs
Medical data consistently shows that ovarian cancer symptoms are present in the early stages. Women just do not recognize them as warning signs. The critical rule is this: if two or more of the following symptoms persist for more than two to three weeks and feel different from your normal, see a doctor.
1. Persistent Bloating
This is the most commonly reported early sign of ovarian cancer. The distinction from ordinary bloating is persistence. Cancer-related bloating does not come and go with meals or your menstrual cycle. It stays. Your abdomen may feel swollen or tight even when you have eaten very little. Some women notice their clothes feel tighter around the waist without weight gain.
2. Pelvic or Abdominal Pain
A dull or sharp ache in the lower abdomen or pelvic region that is not tied to your period deserves attention. This pain can feel like menstrual cramps even when menstruation is weeks away. Some women describe it as a heavy pressure that simply will not lift. Chronic pelvic pain without a clear cause is not normal, regardless of age.
3. Difficulty Eating or Feeling Full Very Quickly
If a normal-sized meal leaves you uncomfortably full after just a few bites, and this happens regularly, it is worth investigating. Ovarian cancer causes fluid buildup in the abdomen and creates pressure on surrounding organs, making eating feel difficult. Loss of appetite that is not explained by stress or illness is also a signal.
4. Frequent or Urgent Need to Urinate
When a growing ovarian tumor presses on the bladder, it can create a frequent urge to urinate or the sensation of needing to go urgently without producing much. This often gets misdiagnosed as a urinary tract infection. If antibiotics provide no lasting relief and the symptom keeps returning, push for a gynecologic evaluation.
5. Unexplained Fatigue
Fatigue caused by cancer is different from tiredness after a busy day. It is a persistent, bone-deep exhaustion that rest does not fix. On its own, fatigue has many causes. But combined with two or three other symptoms on this list, it becomes significant.
6. Lower Back Pain Without a Musculoskeletal Cause
When fluid accumulates in the pelvis or a tumor grows large enough to press against surrounding structures, it can cause persistent lower back discomfort. If your back pain has no injury or posture explanation and does not respond to standard treatment, a gynecologic evaluation is warranted.
7. Changes in Bowel Habits
Persistent constipation, diarrhea, or a noticeable change in how your digestive system functions, without a dietary explanation, can be connected to abdominal tumors pressing on the bowel. Many women attribute this to irritable bowel syndrome or spicy food, delaying investigation.
8. Menstrual Irregularities
Changes in menstrual cycle length, unexpected spotting between periods, or heavier than usual bleeding can sometimes be linked to ovarian cancer in women, particularly if the tumor is affecting the hormone-producing cells of the ovary. Any post-menopausal bleeding should be investigated immediately, with no exceptions.
9. Swelling of the Abdomen
A noticeably swollen abdomen that is not explained by weight gain or diet may be caused by a large tumor or by ascites, which is fluid accumulating in the abdominal cavity. Some women notice their stomach looks visibly distended even while other parts of their body have not changed.
10. Unexplained Weight Loss
Losing weight without trying, particularly when combined with loss of appetite and fatigue, is a pattern associated with several cancers including ovarian cancer. This is not the same as losing a few kilograms after changing your diet. It is weight loss without an explanation.
Important note on persistence: A single symptom that comes and goes is usually not ovarian cancer. The pattern to watch for is multiple symptoms that are new for your body, that stay for more than two to three weeks, and that occur more than twelve times a month. That combination is what studies show most consistently precedes an ovarian cancer diagnosis.
Ovarian Cancer Causes and Risk Factors
No one single cause has been identified. But research has clearly connected several factors to a higher risk of developing ovarian cancer in women.
Genetic Mutations (BRCA1 and BRCA2)
This is the most significant known risk factor. Women with mutations in the BRCA1 or BRCA2 genes face a lifetime risk of ovarian cancer of 44 percent and 17 percent respectively, compared to roughly 1 percent in the general population. These same mutations are strongly connected to breast and ovarian cancer risk together, which is why a family history of breast cancer should prompt a conversation about ovarian cancer screening.
If your mother, sister, or daughter has had breast and ovarian cancer, or if you have had breast cancer yourself, genetic counseling and BRCA testing are worth discussing with your doctor.
Age
Ovarian cancer in women can occur at any age, but risk rises sharply after 40 and peaks between 55 and 64 years. Postmenopausal women account for the majority of diagnoses. However, germ cell tumors can affect girls and young women in their teens and twenties.
Endometriosis
Women with endometriosis, a condition where tissue similar to the uterine lining grows outside the uterus, have a higher risk of certain types of ovarian cancer, particularly clear cell and endometrioid subtypes.
Reproductive History
Women who have never been pregnant have a modestly higher risk than those who have carried a pregnancy to term. Conversely, having multiple pregnancies and breastfeeding are associated with reduced risk.
Hormone Replacement Therapy (HRT)
Long-term use of combined estrogen-progesterone hormone replacement therapy after menopause has been linked to a slightly elevated risk of ovarian cancer. Women considering or currently using HRT should discuss this with their doctor.
Obesity
Excess body weight increases circulating estrogen levels, which can influence ovarian cancer risk. Research consistently links obesity with higher incidence rates, particularly for endometrioid and clear cell subtypes.
Early Menstruation or Late Menopause
Starting menstruation before age 12 or reaching menopause after 55 increases the total number of ovulation cycles over a lifetime, which is associated with higher risk.
Family History
Beyond BRCA mutations, a family history of ovarian, colorectal, or uterine cancer in a first-degree relative increases personal risk and warrants closer monitoring.
India-Specific Statistics Every Woman Should Know
These numbers are not shared to alarm. They are shared because awareness of the scale of this problem is what motivates timely action.
India reports the second-highest number of ovarian cancer cases worldwide, after China, with an age-standardised rate of 6.6 per 100,000 women.
47,333 new cases of ovarian cancer were diagnosed in India in 2022, with 32,978 deaths in the same year.
Ovarian cancer contributes to 6.6 percent of all women’s cancers in India and ranks as the third most common cancer among Indian women after breast and cervical cancer.
70 to 80 percent of Indian patients are diagnosed at an advanced stage (Stage III or IV), primarily because of nonspecific early symptoms, limited awareness, and delayed medical consultation.
The overall 5-year survival rate in India across all stages has historically been around 16 percent, compared to over 50 percent in high-income countries. This gap is almost entirely explained by late-stage diagnosis. It is not a gap in available treatment. It is a gap in early detection.
Women in Mumbai and other metropolitan areas have better access to advanced ovarian cancer treatment than women in rural regions, which is a significant advantage if that access is used at the right time.
Ovarian Cancer Stages: What They Mean and Why Timing Matters
Understanding ovarian cancer stages helps patients and families make sense of what a diagnosis means and what treatment will look like.
Stage I: Cancer Confined to the Ovaries
The cancer has not spread beyond one or both ovaries. Five-year survival rate: above 90 percent. This is the stage at which treatment is most straightforward and outcomes are most favorable.
Stage II: Spread to the Pelvis
Cancer has extended to other pelvic organs such as the uterus or fallopian tubes, but has not reached the abdomen beyond the pelvis. Five-year survival rate: approximately 70 percent.
Stage III: Spread to the Abdomen
Cancer has spread to the lining of the abdomen, the surface of abdominal organs, or nearby lymph nodes. This is where most Indian women are diagnosed. Five-year survival rate: approximately 30 to 40 percent.
Stage IV: Spread to Distant Organs
Cancer has reached the lungs, liver, or other distant organs. Treatment focuses on controlling the disease, managing symptoms, and maintaining quality of life. Five-year survival rate: approximately 17 to 20 percent.
The difference between Stage I and Stage III survival is not primarily about the quality of treatment. It is about when the treatment started. A woman diagnosed at Stage I has a 90 percent chance of being alive in five years. A woman diagnosed at Stage III has roughly a 35 percent chance. The early signs of ovarian cancer described above are the window that determines which stage a woman enters care at.
Ovarian Cancer Diagnosis: What to Expect
If you present to a doctor with persistent symptoms, a responsible diagnostic workup typically involves the following steps.
Pelvic Examination
A physical examination of the reproductive organs to check for any abnormal masses or tenderness. This alone cannot confirm or rule out cancer, but it guides the next steps.
Transvaginal Ultrasound
High-frequency sound waves produce images of the ovaries and nearby structures. This is usually the first imaging tool used when ovarian cancer symptoms are present. It can detect masses, cysts, or tumors and give an initial sense of their size and character.
CA-125 Test for Ovarian Cancer
The CA-125 test measures a protein in the blood called cancer antigen 125. Elevated levels are often found in women with ovarian cancer, making it a useful part of the diagnostic picture.
However, the CA-125 test for ovarian cancer has important limitations. Non-cancerous conditions such as endometriosis, uterine fibroids, pelvic inflammatory disease, and even normal menstruation can also raise CA-125 levels. For this reason, CA-125 is not used as a standalone screening test for the general population.
Where the CA-125 test is most useful: as part of a set of investigations in a woman with symptoms, as a baseline before treatment begins, and as a monitoring tool during and after ovarian cancer treatment to track whether the cancer is responding or returning.
CT Scan or PET Scan
These imaging tests show whether cancer has spread to other organs or lymph nodes, which is essential for staging and treatment planning.
Biopsy
A tissue sample taken from the ovary or surrounding area is examined under a microscope by a pathologist. This gives the definitive diagnosis, identifies the type and grade of cancer, and guides treatment decisions.
Genetic Testing
Women diagnosed with ovarian cancer are now routinely offered genetic testing for BRCA1 and BRCA2 mutations. The result affects treatment choices, particularly the use of targeted therapies. For example, patients with BRCA1 or BRCA2 mutations may benefit from PARP inhibitor therapy, which is a targeted treatment option for ovarian cancer.”
Ovarian Cancer Treatment: Full Overview
Ovarian cancer treatment in Mumbai at a specialized cancer center combines multiple approaches, adjusted to the stage, type, and individual circumstances of each patient.
Surgery
Surgery is the primary treatment for most cases. The extent of surgery depends on the stage:
In early-stage disease, surgery may involve removing only the affected ovary and fallopian tube (unilateral salpingo-oophorectomy). In young women who wish to preserve fertility, this approach can sometimes be used when cancer is limited to one ovary.
In advanced-stage disease, the goal is cytoreductive surgery (also called debulking), which removes as much tumor as possible, including the uterus, both ovaries, fallopian tubes, affected lymph nodes, and any tumor deposits visible in the abdomen.
Chemotherapy
Chemotherapy typically follows surgery and uses intravenous drugs to destroy remaining cancer cells. The standard first-line regimen combines carboplatin and paclitaxel, usually given in six cycles.
For selected patients with advanced disease, HIPEC (hyperthermic intraperitoneal chemotherapy) is offered at specialized centers. This involves delivering heated chemotherapy directly into the abdominal cavity during surgery, targeting cancer cells that are difficult to reach through standard IV chemotherapy.
Targeted Therapy: PARP Inhibitors
For women with BRCA1 or BRCA2 mutations, PARP inhibitors represent a significant advance in ovarian cancer treatment. These drugs block a protein that cancer cells use to repair their damaged DNA, effectively stopping them from replicating. Clinical evidence shows PARP inhibitors can reduce the risk of cancer recurrence by up to 70 percent in women with BRCA-associated ovarian cancer when used as maintenance therapy after initial treatment.
This is one of the most important advances in ovarian cancer care in recent years and is now available at specialized oncology centers in Mumbai.
Immunotherapy
Immunotherapy drugs help the immune system recognize and attack cancer cells. They are increasingly used in cases of recurrent or platinum-resistant ovarian cancer and show promise as part of combination regimens with targeted therapy.
Hormone Therapy
For certain types of ovarian cancer, particularly stromal tumors that respond to hormones, hormone therapy using drugs that block or lower estrogen levels can slow cancer growth.
Radiation Therapy
Radiation is not routinely used as a primary treatment for ovarian cancer in the way it is for other cancers, but it may be used in selected situations to treat localized recurrence or to manage symptoms.
Prevention: How to Lower Your Risk of Ovarian Cancer
There is no guaranteed way to prevent ovarian cancer. But several factors are linked to meaningfully lower risk, and they are all within reach of most women.
Oral Contraceptives
Women who have used oral contraceptive pills for five or more years have been shown to have a 40 to 50 percent lower risk of ovarian cancer compared to women who have never used them. The protective effect persists for years after stopping. This is one of the most consistent findings in ovarian cancer epidemiology. Women should discuss the benefits and risks of oral contraceptives with their doctor.
Pregnancy and Breastfeeding
Each full-term pregnancy reduces ovarian cancer risk, and breastfeeding provides additional protection. The biological mechanism relates to the reduced number of ovulation cycles over a lifetime.
Tubal Ligation and Oophorectomy
In women at average risk, tubal ligation (having the fallopian tubes tied) is associated with a reduced risk of ovarian cancer. In women at very high risk due to BRCA mutations, prophylactic removal of the ovaries and fallopian tubes (bilateral salpingo-oophorectomy) dramatically reduces risk and is a medically established preventive option.
Genetic Counseling and Testing
Women with a family history of breast and ovarian cancer should consider genetic counseling. Knowing your BRCA status allows you and your doctor to make informed decisions about surveillance, preventive interventions, and family planning.
Healthy Body Weight
Maintaining a healthy weight reduces circulating estrogen levels and is associated with lower cancer risk across multiple cancer types, including ovarian cancer in women.
Avoiding Talc in the Genital Area
Some studies have linked long-term use of talcum powder in the genital area with a modest increase in ovarian cancer risk. Avoiding this practice is a simple precaution.
Diet and Nutrition: What the Research Says
Diet alone cannot prevent ovarian cancer. But the evidence consistently shows that what women eat influences cancer risk and, for those already diagnosed, affects treatment outcomes and survival.
Foods That May Lower Risk
Cruciferous vegetables such as cauliflower, cabbage, broccoli, and mustard greens contain compounds called glucosinolates that have shown cancer-protective properties in research. A study of 675 women with ovarian cancer found that women who consumed the highest amounts of cruciferous vegetables had the lowest risk of developing the condition, with risk decreasing with every ten additional servings per month.
Fruits and vegetables broadly, particularly those rich in antioxidants like tomatoes, carrots, sweet potatoes, and citrus, help protect cells from oxidative damage that can trigger abnormal growth.
High-fiber foods including whole grains, legumes, and vegetables support digestive health, reduce inflammation, and help maintain hormone balance.
Green tea contains polyphenols that have shown anti-tumor properties in laboratory studies, though clinical evidence in humans is still emerging.
One analysis found that women who follow a healthier diet after an ovarian cancer diagnosis experience a 14 percent reduction in mortality compared to those who do not make dietary changes.
Foods to Limit or Avoid
Processed meats, red meat in excess, refined sugars, and highly processed packaged foods are consistently linked to higher inflammation and poorer outcomes in cancer research. During ovarian cancer treatment, greasy foods often worsen nausea and fatigue, particularly during chemotherapy cycles.
This does not mean strict elimination. A practical approach: build meals around vegetables, whole grains, lean protein (like lentils, legumes, fish, and chicken), and healthy fats. Reduce processed foods as a category rather than obsessing over individual ingredients.
After Treatment: Monitoring for Recurrence
One of the sections that most ovarian cancer blogs skip entirely is what happens after treatment ends. For women who complete surgery and chemotherapy and achieve remission, the journey is not over. Recurrence is a genuine risk, and monitoring for it is part of responsible long-term care.
Routine follow-up appointments with your oncologist are typically scheduled every three months for the first two years, then every six months for three more years, and annually after that.
CA-125 monitoring is used as a marker during follow-up. A rising CA-125 level after successful treatment can be an early indicator of recurrence, often before symptoms develop.
Imaging scans are used when CA-125 rises or when new symptoms appear.
Women who experience recurrence are not out of options. Second-line chemotherapy, PARP inhibitors, immunotherapy, and other targeted treatments are available, and outcomes for recurrent ovarian cancer continue to improve as new therapies enter practice.
Patients with BRCA mutations who were not offered PARP inhibitor maintenance therapy after initial treatment should ask their oncologist whether this option is now appropriate for them.
Myths vs Facts About Ovarian Cancer
Myth: Ovarian cancer always shows obvious symptoms.
Fact: The early signs of ovarian cancer are subtle and easy to attribute to other causes. There are no dramatic early symptoms. Persistent, low-grade symptoms that last more than two to three weeks are the signal to act on.
Myth: A normal Pap smear means you do not have ovarian cancer.
Fact: The Pap smear screens for cervical cancer, not ovarian cancer. These are two completely different cancers. A normal Pap result gives no information about ovarian cancer risk or presence.
Myth: Only older women get ovarian cancer.
Fact: While risk increases with age and peaks between 55 and 64, ovarian cancer in women can occur at any age. Germ cell tumors, for instance, are more common in teenagers and young adults.
Myth: The CA-125 test is a reliable screening tool for all women.
Fact: The CA-125 test for ovarian cancer is useful as part of a diagnostic investigation in women with symptoms, and as a monitoring tool during and after treatment. It is not reliable as a standalone screening test for the general population because many non-cancerous conditions also raise CA-125 levels.
Myth: If ovarian cancer runs in your family, there is nothing you can do.
Fact: Women with a family history of breast and ovarian cancer, or with confirmed BRCA mutations, have real options: closer surveillance, preventive surgery, oral contraceptives, and lifestyle modifications. Genetic counseling turns a family history from a source of anxiety into a basis for informed action.
Myth: Ovarian cancer is always fatal.
Fact: When diagnosed at Stage I, the five-year survival rate exceeds 90 percent. Even at later stages, advanced treatments including targeted therapy, PARP inhibitors, and immunotherapy have significantly improved outcomes. This is a serious cancer, but it is not automatically a death sentence.
When to See a Doctor: Your Action Checklist
Do not wait for symptoms to become unbearable. If you experience two or more of the following for more than two to three weeks, make an appointment with a gynecologist:
- Bloating that does not resolve with diet changes
- Pelvic or lower abdominal pain not related to your period
- Feeling full very quickly or loss of appetite
- Urinary urgency or frequency that is new for you
- Back pain with no musculoskeletal explanation
- Unexplained changes in bowel habits
- Post-menopausal bleeding of any amount
When you see your doctor, be specific about duration. Ask directly about a pelvic examination, transvaginal ultrasound, and CA-125 test. If your concerns are dismissed without investigation and symptoms persist, seek a second opinion from a gynecologist for ovarian cancer in Mumbai who specializes in gynecologic oncology.
What services or treatment women with ovarian cancer get at Zynova Shalby Hospital:
A team of experienced ovarian cancer specialist doctors in Mumbai who manage all stages and types of ovarian cancer, including high-grade serous carcinoma and rare subtypes. A dedicated gynecologist for ovarian cancer in Mumbai for every patient, working alongside medical oncologists, radiation oncologists, and pathologists. Advanced diagnostic services including high-resolution transvaginal ultrasound, CA-125 testing, CT and PET scanning, and molecular pathology for accurate staging and treatment planning. Modern surgical techniques including minimally invasive laparoscopic surgery and robotic-assisted procedures for faster recovery with fewer complications. Access to PARP inhibitors and other targeted therapies for women with BRCA mutations, integrated into individualized treatment plans. Post-treatment surveillance programs with structured follow-up schedules and ongoing CA-125 monitoring to detect recurrence early. A patient-centered approach that includes fertility preservation discussions for younger women, nutritional guidance during chemotherapy, and psychological support for patients and families.
Zynova Shalby Hospital is the best cancer hospital in Mumbai for women who want expert, multidisciplinary care in one place, without the exhausting experience of navigating multiple specialists on their own.
To book a consultation with an ovarian cancer specialist at Zynova Shalby Hospital, contact the hospital directly.
Conclusion
Ovarian cancer symptoms are not invisible. They are just easy to explain away. Bloating, pelvic discomfort, feeling full quickly, urinary changes: these are the signals the body sends, sometimes months or even years before a diagnosis is made at a stage when treatment is much harder.
The difference between a Stage I diagnosis and a Stage III diagnosis is not luck. It is often a woman who paid attention, described her symptoms accurately, and found a doctor who took them seriously.
If something in your body has changed and stayed changed, trust that. Book an appointment. Ask about the CA-125 test for ovarian cancer. Ask about a transvaginal ultrasound. If you have a family history of breast and ovarian cancer, ask about genetic testing.
And if you are in Mumbai and want access to experienced ovarian cancer specialist doctors who bring surgery, oncology, diagnostics, and follow-up care together in one place, Zynova Shalby Hospital is here. As the best cancer hospital in Mumbai for gynecologic oncology, the team at Zynova Shalby is equipped to guide you from your first concern all the way through treatment and beyond.
Your health is worth acting on early.
Frequently Asked Questions
What are the very first symptoms of ovarian cancer?
The most common early signs of ovarian cancer are persistent bloating, pelvic or abdominal discomfort, difficulty eating or feeling full quickly, and urinary urgency. These symptoms are nonspecific, which is why many women dismiss them. The pattern to watch for is multiple symptoms that are new and that persist for more than two to three weeks.
Is the CA-125 test accurate for detecting ovarian cancer?
The CA-125 test for ovarian cancer is useful but not definitive on its own. It is part of a broader investigation that includes pelvic examination, ultrasound, and imaging. CA-125 can be elevated in non-cancerous conditions, so a high result does not confirm cancer and a normal result does not rule it out.
What ovarian cancer stages have the best survival outcomes?
Stage I has the best prognosis, with a five-year survival rate above 90 percent. This drops significantly at Stage III and IV, which is why acting on early symptoms before the cancer spreads is so important.
Can ovarian cancer come back after treatment?
Yes, recurrence is a real possibility, which is why structured follow-up care matters. Regular CA-125 monitoring and imaging after treatment allow doctors to detect recurrence early, when additional treatment options are more effective.
Are breast cancer and ovarian cancer related?
Yes. Breast and ovarian cancer share a genetic link through BRCA1 and BRCA2 mutations. Women who have had breast cancer or have a close relative with breast or ovarian cancer have a higher risk of developing ovarian cancer and should discuss genetic testing with a specialist.
How do I find the best gynecologist for ovarian cancer in Mumbai?
Look for a gynecologic oncologist with specific experience in ovarian cancer surgery, access to advanced diagnostics including the CA-125 test, and a multidisciplinary team. Zynova Shalby Hospital offers all of this under one roof. Contact the hospital to schedule a consultation.
Can ovarian cancer be prevented?
There is no guaranteed prevention, but risk can be meaningfully reduced. Oral contraceptive use for five or more years is associated with 40 to 50 percent lower risk. Maintaining a healthy weight, eating a diet rich in vegetables and fiber, and genetic counseling for high-risk women all contribute to risk reduction.
Leave a Comment